 B. A. Badie, M.D.
B. A. Badie, M.D.
“I have known that I would be a physician since I was very young. While I enjoy practicing medicine in the fields of allergies and asthma, it is really the welfare of and interaction with my patients that matters to me the most. My patients have always been a part of my professional family, and as such, it is my goal to always treat the patient, rather than just the disease. Having practiced medicine in the Denton area for over 35 years, I have had the pleasure and privilege of watching many of my patients grow up, go to college, and bring their own children back to see me. The best compliment for a physician is when a patient refers another member of their family or friend to him as a patient.”
Dr. Badie has been practicing Denton area since 1976 and is a board certified allergist. He specializes in the care of children and adults with allergies, asthma, and immune problems. His areas of interest include asthma, sinus disease and skin allergies and he has published multiple scientific articles in the field of allergy.
Diplomate
American Board of Allergy and Immunology
Medical School
M.D., Tehran University, Tehran, Iran
Internship
Detroit Medical Center, Detroit, Michigan
Residency
Pediatrics, William Beaumont Medical Center, Royal Oaks, Michigan
Fellowship
Allergy and Immunology, Louisiana State University and Tulane University Medical Schools, New Orleans, Louisiana
Other Credentials
Clinical Professor of Medicine and Director of Division of Allergy, Qingdao University College of Medicine, Qingdao, China
Director of China-America Asthma Center
Past President of the Denton County Medical Society
Oral immunotherapy / OIT
Our physicians are among a select group of doctors in the United States with extensive experience in oral food desensitization. Our physicians have over 10 years of shared experience with oral immunotherapy. They have successfully desensitized patients of all ages to allergenic foods including peanuts, tree nuts, milk, eggs, soy, wheat and shrimp. In our oral immunotherapy program, the concerning food item is gradually reintroduced, starting with tiny doses and increasing slowly to the full dose over the course of 4-6 months. This form of immunotherapy is conducted only under close medical supervision in our clinic with weekly office visits and oral challenges. Our physicians can evaluate for food allergy and determine whether oral immunotherapy should be considered.
Contact
Dr. B.A. Badie
North Texas Allergy & Asthma Center
Denton North: 2617 Scripture Street, Suite 101, Denton, Texas 76201
Phone: (940) 382-4142
Denton South: 3105 Colorado Boulevard, Suite 101, Denton, Texas 76210
Phone: (940) 387-1700
Fax: (940) 382-7620
info@northtexasallergy.com
http://northtexasallergy.com/
North Texas Allergy & Asthma Center: Dr. Roshni Kandyil Foster, Dr. Samuel Foster and Dr. B.A. Badie
OIT Details
State: Texas
Treats single/multi allergens at once: Single
Offers SLIT for food allergens: No
Additional Features:
Articles in Our Research & Learn Center
There are no knowledge base articles.
Map to Office(s)
[property_map1]
[property_map2]
[property_map3]
[property_map4]
[property_map5]
 Visit
Visit  Any of the
Any of the  It’s an amazing, soap-opera style story of lives transformed by doctors willing to pioneer therapies to counter the clinically-proven diminished quality of life food allergy families. Contrasted with the attempts of organizations like FARE, publications like Allergic Living, and many Facebook food allergy support group “leaders” who deny it’s success and safety and that it is spreading like wildfire across the country. Families want this treatment NOW.
It’s an amazing, soap-opera style story of lives transformed by doctors willing to pioneer therapies to counter the clinically-proven diminished quality of life food allergy families. Contrasted with the attempts of organizations like FARE, publications like Allergic Living, and many Facebook food allergy support group “leaders” who deny it’s success and safety and that it is spreading like wildfire across the country. Families want this treatment NOW.  ABOUT US
ABOUT US We set this site up because the at-large allergist community has failed us. OIT has been around for YEARS and it is well-known and well-documented it produces desensitization. We are under the care of board-certified allergists who take this responsibility very seriously. Read about them on this site to reassure yourself they are not quacks, or storefront Botox peddlers. What they ARE is amazing human beings and healing physicians. They “doctor.” They use their smarts, brains and scientific training to help children with food allergies live normal, full lives without the crippling fear of accidental food ingestion.
We set this site up because the at-large allergist community has failed us. OIT has been around for YEARS and it is well-known and well-documented it produces desensitization. We are under the care of board-certified allergists who take this responsibility very seriously. Read about them on this site to reassure yourself they are not quacks, or storefront Botox peddlers. What they ARE is amazing human beings and healing physicians. They “doctor.” They use their smarts, brains and scientific training to help children with food allergies live normal, full lives without the crippling fear of accidental food ingestion. We also set up this website because the food allergy organizations like FARE and their parent support groups have failed us. We’ve been “beat up”, yelled at, had our comments deleted and been banned from support groups for talking about OIT and how it has saved our kids. Why be in a food allergy support group if they never tell you how you can get rid of it? That there is HOPE! That thousands of children and adults are safely “getting rid” of their once life-threatening food allergies. Even magazines like
We also set up this website because the food allergy organizations like FARE and their parent support groups have failed us. We’ve been “beat up”, yelled at, had our comments deleted and been banned from support groups for talking about OIT and how it has saved our kids. Why be in a food allergy support group if they never tell you how you can get rid of it? That there is HOPE! That thousands of children and adults are safely “getting rid” of their once life-threatening food allergies. Even magazines like  What you do with the oral immunotherapy information is up to YOU. And your doctor. You will be amazed when you encounter an OIT board-certified allergist and get a second opinion. Enjoy your time on the site and hopefully it answers your questions well. We know how you feel and what you want to know because we’ve answered it already hundreds of times.
What you do with the oral immunotherapy information is up to YOU. And your doctor. You will be amazed when you encounter an OIT board-certified allergist and get a second opinion. Enjoy your time on the site and hopefully it answers your questions well. We know how you feel and what you want to know because we’ve answered it already hundreds of times. “Private Practice OIT” Facebook group
“Private Practice OIT” Facebook group A little history: When Liseetsa Mann started the
A little history: When Liseetsa Mann started the  Liseetsa shared all her knowledge, happy to have found a “tribe” of like-minded parents: those who wanted a better life for their food-allergic children. She became a “Pied Piper” of sorts, and began seeking and finding new OIT allergists and creating her famous “list.” Only doctors who met the standards set by Dr. Nash were included. Not just great doctors, but great human beings. Friendly office staff. Nowhere she would not take her own children. She coached and cheered and comforted OIT parents on late night calls, advocated and helped with any and all problems. Word spread.
Liseetsa shared all her knowledge, happy to have found a “tribe” of like-minded parents: those who wanted a better life for their food-allergic children. She became a “Pied Piper” of sorts, and began seeking and finding new OIT allergists and creating her famous “list.” Only doctors who met the standards set by Dr. Nash were included. Not just great doctors, but great human beings. Friendly office staff. Nowhere she would not take her own children. She coached and cheered and comforted OIT parents on late night calls, advocated and helped with any and all problems. Word spread. As members shared “
As members shared “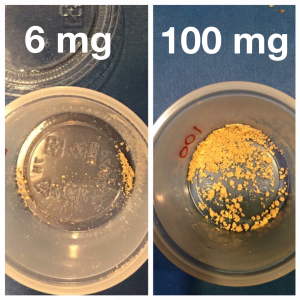
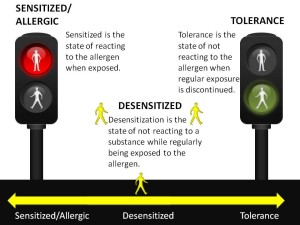 From the literature there is overwhelming evidence that OIT will induce desensitization, meaning that the patient will be able to ingest/be exposed to the food without any reactions. There are over 175 medical journal articles published since 1908 on OIT, as you can see in our Research & Learn Library. Studies have been conducted worldwide, by many different institutions, using many different protocols, methods and different allergenic foods. The results are very consistent in producing desensitization for the majority of participants.
From the literature there is overwhelming evidence that OIT will induce desensitization, meaning that the patient will be able to ingest/be exposed to the food without any reactions. There are over 175 medical journal articles published since 1908 on OIT, as you can see in our Research & Learn Library. Studies have been conducted worldwide, by many different institutions, using many different protocols, methods and different allergenic foods. The results are very consistent in producing desensitization for the majority of participants.
 Some patients who do not especially like the taste of the allergenic food choose not to deliberately consume it, but no longer worry about reading labels. In some instances the patient or parent will choose to shorten the therapy and bring the protection only up to protect against accidental exposures. This is sometimes referred to as “bite-proof:” safety from an accidental bite of something containing the allergen, or eating something that was cross-contaminated with the allergen.
Some patients who do not especially like the taste of the allergenic food choose not to deliberately consume it, but no longer worry about reading labels. In some instances the patient or parent will choose to shorten the therapy and bring the protection only up to protect against accidental exposures. This is sometimes referred to as “bite-proof:” safety from an accidental bite of something containing the allergen, or eating something that was cross-contaminated with the allergen. B) No patient is “too severe.”
B) No patient is “too severe.” What food allergies can be treated with OIT?
What food allergies can be treated with OIT? To date, OIT is the only “proven” method of treating food allergies. It is one of the best studied, most effective, inexpensive and most accessible forms of treatment. Other methods under study and clinical trials include Pre-OIT SLIT, SLIT (Sublingual immunotherapy ), EPIT via the Viaskin patch (epicutaneous immunotherapy), and immunotherapy with attenuated food proteins or peptides (rather than the whole food).
To date, OIT is the only “proven” method of treating food allergies. It is one of the best studied, most effective, inexpensive and most accessible forms of treatment. Other methods under study and clinical trials include Pre-OIT SLIT, SLIT (Sublingual immunotherapy ), EPIT via the Viaskin patch (epicutaneous immunotherapy), and immunotherapy with attenuated food proteins or peptides (rather than the whole food). “It’s coming” has been said for 15+ years now. If you need long-term proof, then OIT will have to be your choice since it is the only thing that has been studied for many years. The other food allergy treatments either have no results on humans, or are not very effective, or will be put on the market with “FDA approval” with a small study of a few hundred people for a max of 3 years. No long-term safety or effectiveness data whatsoever.
“It’s coming” has been said for 15+ years now. If you need long-term proof, then OIT will have to be your choice since it is the only thing that has been studied for many years. The other food allergy treatments either have no results on humans, or are not very effective, or will be put on the market with “FDA approval” with a small study of a few hundred people for a max of 3 years. No long-term safety or effectiveness data whatsoever. 1) Is the risk of OIT less (or equal) than not doing it (risk vs. benefit)? Compare versus the risks of “strict avoidance” and its well-published failures.
1) Is the risk of OIT less (or equal) than not doing it (risk vs. benefit)? Compare versus the risks of “strict avoidance” and its well-published failures.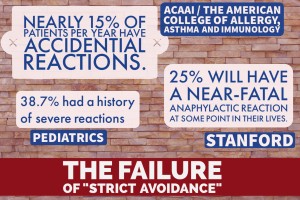 Here are the facts about the “risks” of not doing treatment and choosing a path of “Strict Avoidance”. These are REAL odds, and in addition you have to live on hyper-alert, deal with exclusion and social/family/school stress and food fear:
Here are the facts about the “risks” of not doing treatment and choosing a path of “Strict Avoidance”. These are REAL odds, and in addition you have to live on hyper-alert, deal with exclusion and social/family/school stress and food fear: There are multiple studies going back more than a decade that quantify the stress for food allergic families. There are several studies that show the positive impact OIT has, not only on the food allergic person, but the whole family, including caregivers:
There are multiple studies going back more than a decade that quantify the stress for food allergic families. There are several studies that show the positive impact OIT has, not only on the food allergic person, but the whole family, including caregivers: You can hear
You can hear  No! OIT must always be done under the care of board-certified allergist who has trained to perform this treatment. No pediatricians, family doctors, ENT’s, chiropractors, licensed acupuncturists, or well-meaning family members should ever give a food-allergic child their allergen.
No! OIT must always be done under the care of board-certified allergist who has trained to perform this treatment. No pediatricians, family doctors, ENT’s, chiropractors, licensed acupuncturists, or well-meaning family members should ever give a food-allergic child their allergen. Is OIT covered by insurance?
Is OIT covered by insurance? 1) Learn about OIT: Spend time learning about how OIT works. Visit our
1) Learn about OIT: Spend time learning about how OIT works. Visit our  It is understandable that a child (and his/her parents) would have a certain level of anxiety when faced with the prospect of deliberately ingesting a food allergen. What we see is that both parents and kids have a natural, normal negative response to the idea of OIT! Always! No one ever says, “Oh yeah, sounds great, sign me up Mom.”
It is understandable that a child (and his/her parents) would have a certain level of anxiety when faced with the prospect of deliberately ingesting a food allergen. What we see is that both parents and kids have a natural, normal negative response to the idea of OIT! Always! No one ever says, “Oh yeah, sounds great, sign me up Mom.” What is the timeline for food desensitization?
What is the timeline for food desensitization? What do we bring to the Day1/ rapid desensitization appointment?
What do we bring to the Day1/ rapid desensitization appointment? Here’s a study published in 2009
Here’s a study published in 2009  How long should we expect to be in the office during “updose” visits?
How long should we expect to be in the office during “updose” visits? Of course! Pursuing food desensitization doesn’t mean that the rest of your life gets put on hold. You work OIT into your life, not work your life around OIT.
Of course! Pursuing food desensitization doesn’t mean that the rest of your life gets put on hold. You work OIT into your life, not work your life around OIT.
